Discussion with Dr. Chris Clagett
risk, benefit, health, and trust


Dr. Chris Clagett served in the U.S. Navy for 34 years retiring in 2019. Several of the latter years of his military career, Chris worked as the chief of preventive medicine. The Navy and Marine Corps Force Health Protection Command website describes the role of preventive medicine as follows:
We provide force health protection enhancement of organic preventive medicine assets and rapid assessment of health threats in a theater of operations with the objective of either prevention or control. We also support Navy medical leaders who make Navy preventive medicine policy and medical department personnel who identify, evaluate, monitor, and respond to diseases, injuries, and environmental factors that threaten human health.
Chris was kind enough to walk me through how to assess risk of infectious disease to the military force using SARS-CoV2 as a case example. We also discuss any potential benefit of chemoprophylaxis in the same context. The discussion is available on youtube where you can see supporting graphs used to illustrate various points and also on spotify, apple, podbean etc. I’ll provide a brief summary of the discussion here, then some closing thoughts about the state of the medical establishment and implications for optimizing health and fitness in the military setting.
Establishing Risk
Early in the conversation Chris makes it clear that to establish risk, overall deaths is a useless metric. The information needed most urgently is the Infection Fatality Rate (IFR). In other words, the likelihood of death with any given infection. He then shares the data allowing an estimation of this figure stratified by age so that we can focus on the overall risk for the military demographic.
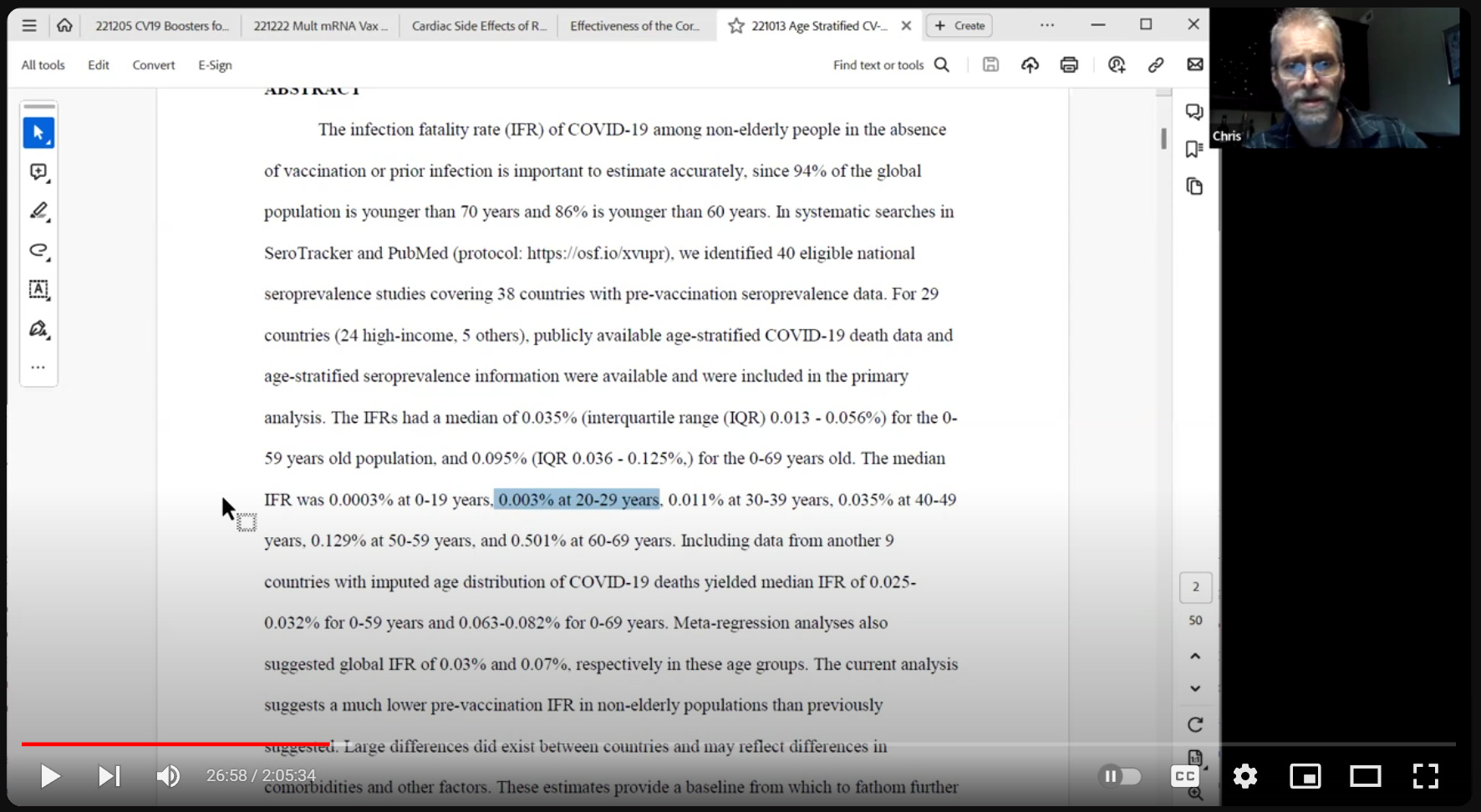
As can be seen, for the 20-29 demographic that comprises the majority of the military, the IRF is .003%. That leads us to discuss other factors known to have increased the IFR for SARS-CoV2. While many co-factors have been established, obesity emerged as one of the most relevant dramatically increasing the IFR. It is salient to note here that military regulations set at upper limit for allowable bodyfat percentage resulting in a much lower rate of obesity in that population as compared to the population at large. This suggests that the .003% figure overestimates the IFR in the military population. Considering additional co-factors that disqualify individuals from military service, such as severe autoimmune conditions, only compound this effect. The bottom line Chris comes away with having served at the highest levels tasked with assessing risk and preventing harms from infectious disease to the military population is that the risk posed by SARS-CoV2 on the majority of military personnel was essentially negligible.
Assessing Benefit When Risk is Negligible
Chris goes on to make the point that assessing the benefit of any given intervention is essentially impossible when risk is negligible. Given the IFR in ages under 29, prophylactic interventions simply couldn’t reduce the risk of death.1 If there is no benefit, then the risk-benefit calculation becomes meaningless as we’re left to determine the overall risk of the treatment in question, which is all downside. In the case of these mRNA gene therapies, Chris discusses how one of the clearest and most obvious risks given the data is increased risk of infection with SARS-CoV2! Oh, the irony…

Treating Spike Protein as an Allergen
In a study examining IgG concentrations relative to number of mRNA dosages it was discovered that continued vaccination dramatically increases IgG4 concentration. This is significant because IgG4 functions to downregulate immune response to a given antigen, in this case, the cytotoxic spike protein. With the ability of the immune system to target this antigen so modulated, we would expect to see infections by the pathogen carrying this antigen to increase. As it turns out, this is exactly what we see.
Infections Highly Correlated to Vaccination
The more doses of mRNA received, the higher the incidence of COVID-19. Not only did claims that these treatments would prevent infection not pan out, they were exactly the opposite of what has been observed. Chris demonstrates this by displaying a graph from a study showing a strong positive correlation between dose and infection where there is a clean doubling of infection risk for those “fully vaccinated” compared to the unvaccinated population investigated.

I can’t help but note the youtube tag to check out the latest info from the CDC on the COVID vaccine. Lets take a break to see what they have to say.

Wow. 6 months and older. The population with a .0003 IFR. Unconscionable… but I digress.
mRNA Doses vs. All Cause Death
If no possible benefit and a clear increase in infections isn’t bad enough, following our discussion, Chris sent me the following charts in a GIF assembled from UK data. They show that those who have received more doses of the mRNA treatments are dying at higher rates than the unvaccinated over time.

Aside from this troubling data, we of course have vaccine injury surveillance data from across the world showing a wide range of issues, some of which we discussed. Given the data from active surveillance in Australia suggesting a 3% rate of serious adverse events, an increase in all cause mortality associated with dosage over time is hardly surprising.
Applications to Holistic Health and Fitness
The main takeaway here is that if you want to make informed risk decisions to reach your goals and support a healthy lifestyle, you can’t afford to trust captured institutions such as the CDC. It is also important to note that the more powerful an institution is, the more likely it has been completely captured by interests not aligned with your own. To appreciate the disturbing scale and scope of this phenomenon, this presentation from the perspective from high profile venture capitalist Bill Gurly is indispensable. Regulatory capture is a rule proving itself to be extremely resistant to exceptions.
Trust and Discernment
So who can you trust? Only you can answer that question. Discernment is key, and is likewise a skill that takes time and effort to develop. Trust is a risk decision. Unlike the mRNA gene therapies, there is upside potential for taking a risk to trust. Trust opens the door to opportunities, and it can save valuable time if you take the advice of someone worthy of that trust. The better your discernment, the more favorable your risk-benefit ratio is in any given trust decision. The process of developing discernment is complex and nuanced. I won’t go into my process here. What I will include however, is a heuristic I’ve adopted to aid my own discernment in these trying times of MindWar: I will never fully trust the health advice of someone who recommended these novel gene therapies for young and healthy individuals. I’ll consider their recommendations if they’ve proven competent in a specialized field, but only with full evidence and reasoning provided to support. I’ll also probably apply more scrutiny to such an individual than usual. To take the recommendation of someone who failed so spectacularly in this regard on faith is to abdicate the responsibility you bear for maintaining your own health and wellbeing.
Responsibility for Health
If military medicine is to ever again earn trust writ large, those who coerced this treatment on the population must be held accountable. Not only was the order illegal, at this point it is clear significant medical harms have resulted. Even if there had been benefit, the unlawful manner by which service members were coerced into taking these products would have been unacceptable. That net death and injury has been a consequence is outrageous. That there has been no accountability for these failures has only severed trust between members of the Armed Forces and military medicine writ large. In an effort to begin to restore this decimated trust, current and former service members such as Dr. Clagett, Dr. Long, Dr. Chambers, Dr. Sigoloff, and myself are calling for accountability. Regardless of whether or not this call for accountability is ultimately met with success, it must be recognized that nobody will ever care more about your health than you. It is your responsibility to understand this and act accordingly. Competent medical professionals will be able to explain risks and benefits in a manner that you will find persuasive, or they won’t. Now more than ever, the onus is on medical providers to do so. If unwilling or unable, they aren’t worthy of my trust. Only you can decide if they’re worthy of yours.
This was demonstrated in phase II clinical trials for Pfizer bnt162b2 where the mostly young and healthy population included demonstrated 23% more overall deaths in the treatment arm.
Great post! One of the best I’ve read on the scamdemic. Thanks especial for the risk/reward discussion and the due diligence tips. Most Americans don’t “get” the risk/reward concept for medical interventions. It’s all “magic goodness.” Secondly, most don’t have any inkling of the failings, tricks, and errors of the “expertocracy.” Once you “see” risk/reward and the intentionally wrong advice of the experts , you can’t unsee them... and there goes your trust. I know from experience that’s a painful, foundation shattering awakening. I’m afraid most folks don’t want to go there as they intuitively know the vertigo that awaits.
Grant understood me correctly. IFR is a [relatively!] easily-measured proxy for infection severity. You are also right that death is not the only downside of Covid, and I have never claimed that it was. But aggregating all the other downsides of Covid is an impossibility, so it is necessary that we use a metric that both has some real world meaning and is feasible to measure. The young, especially in the healthier-than-average military population, almost never have a hard time with SCV2. And the 3 per 100,000 among the 20-29 year olds who do have some good reason for it. I suspect that the low double digit deaths the DoD attributes to Covid were service members who either had a coincidental infection while dying of something else or their PCR was a false positive. False positive PCRs are something we hardly discuss. They can be caused by the amplification of viral debris left over from a previously cleared recent infection (up to 60 days) or they can even be caused by non-specific binding of the primer to a nucleotide sequence similar to the target sequence. It is necessary to confirm that the PCR amplicon actually corresponds to a known nucleotide sequence of the virus. This last step is almost never done.
My second bout of frankenvirus was a little rough. Fevers, chills, baaad body aches, cough. Needed ivermectin for that; started IVM on symptom day 3 and was 95% resolved in 18 hrs. No 30 year old would have had my experience.