


One of the reasons I decided to get into physical therapy was the recognition that a lot of folks seeking medical care are doing so for musculoskeletal (MSK) injuries that primary care docs can’t really do much to help with. People get injured… a lot. You would think if you get injured you could go to your doctor and get some good advice, but this isn’t a particularly astute assumption. In primary care they need to make sure you aren’t dying, then refer you to a specialist if they don’t think you’ll get better on your own. This isn’t an easy process, there are a lot of systems that need to be checked and countless specialists that might end up being most appropriate. The MSK system being highly amenable to conservative care, your primary care doc will typically write a prescription for a non-steroidal anti-inflammatory medication (NSAID) such as ibuprofen and say something like “keep off it”. If they’re really squared away they might print off a therapeutic exercise handout that roughly corresponds to a common diagnosis for the region. Low back pain? Here’s some meds and a list of stretches. Oh, I read yoga helps too, why not try that? You sprained your ankle? Wow, that’s a lot of swelling, you should definitely use the RICE (rest, ice, compression, elevation) protocol! Fortunately, most people will get better in spite of this weak sauce advice.

Since physical therapy is one of the specialties that primary care can refer to, they might decide to send you on over, especially if pattern recognition tells them you’ll be back in a couple months complaining of the same thing. But what does a physical therapist even do?

Ask a dozen PTs and you’ll probably get a dozen answers. Some say we’re movement specialists, others say we’re the non-surgical MSK experts (I like this one, personally). Practically, we all approach treatment in our own unique ways. Most PTs will conduct an exam, find out what your goals are, identify physical impairments, then develop a plan for how to address those impariments to help you reach your goals. Methods for addressing identified impairments vary wildly. Some PTs have everyone sit on foam rollers, some are manual therapy gurus, some will run you through the algorithms of mechanical based diagnosis and treatment, and others will put acupuncture needles in you with or without some added electric current. I like to load patients optimally. I think a great many legit PTs would agree that it all comes down to optimal loading, and justify all of the aforementioned practices as a way to get after optimal loading, but I think you can almost always get by without soft tissue work and modalities and cut right to the chase. I could be wrong. In any case you’re here because you’re interested in my opinion, so suffice it to say this is something that would be debated amongst PTs, and almost anything can be rationalized, even if I might think it’s a waste of time.
Before getting into what constitutes optimal loading we need to define injury and healing. So what is injury? I think of it as a condition where a given tissue’s tolerance to load has been exceeded. This can happen all of the sudden, or gradually over time. Those all of the sudden injuries are called acute injuries, think falls, trips, slips etc. If we were to look at such an injury on a graph, it would look something like this:

The other main category of injuries to consider are those that are sustained gradually over time. We generally call these overuse injuries (think running too many miles too many days with too little rest). If we were to graph an overuse injury, it would look something like this:

So this is basically what injury looks like. Tissue load tolerance gets exceeded causing a loss of structural integrity. In tendon and muscle this is called a strain. In ligaments this is called a sprain. When bone tissue tolerance is exceeded gradually over time this is called a bone stress injury (BSI). Stress fractures are BSIs, and they can progress to frank fractures. Bone can obviously also fracture all of the sudden in an acute injury. Other tissue such as labrum in the shoulder and hip joints and meniscus in the knee can be torn. In many cases these injuries will heal without the need for surgical intervention, but some conditions generally warrant a referral to an orthopedic surgeon e.g. displaced fractures, grade 3 ACL sprains etc. A good PT will know what has good conservative rehab potential given a patient’s profile and goals and what doesn’t.
Now that we covered injury, what is healing? That is a bit more complicated. The physiological processes that contribute to tissue healing are legion. That said, healing tends to occur logarithmically with a whole lot of tissue tolerance being recovered early on, then a frustratingly long time to get to 100% of where the tissue can hope to get to. The timeframe will vary widely depending on the tissue. A highly vascularized tissue like muscle will get 80% “healed” after a grade 2 strain in 4-6 weeks. To give you an idea of how that logarithmic function works, getting above 95% “healed” in this case could take over 4 months. For a poorly vascularized tissue like acetabular labrum that same 80% might take 6-9 months with 95%+ taking 2-3 years.
As you can see, healing takes time. Everyone wants to speed this process along, and a lot of treatment is understood to accomplish this. RICE, NSAIDs, and soft tissue work or even corticosteroids might alleviate pain, but they won’t accelerate this process. In fact, if we want to try to be rational we might expect that these analgesic treatments that inhibit the inflammatory response might make the healing process take even longer. The literature on this is pretty equivocal, but I don’t think there is any way these things don’t impair/delay healing. Patients don’t want to hear this, and neither do providers. We all want that quick fix, but there really isn’t one. There is a slow fix though! Enter optimal loading.

It turns out mechanical loading is required for a constellation of physiological functions that result in the repair and strengthening of tissue. This occurs without injury as well, but is especially important in the context of injury to ensure that tissue heals in a way that contributes to optimal function. The mechanical loading provides essential information to the system to ensure that this tissue will be able to handle these imposed demands at higher magnitudes in the future. So what does optimal loading look like in the rehab context? Lets look at a crude graph I drafted to illustrate:
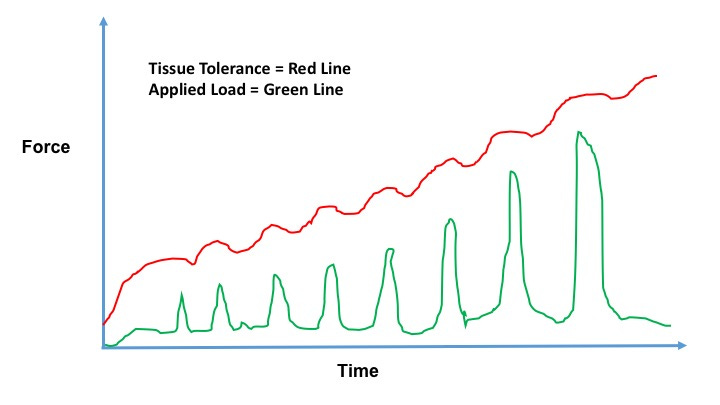
Consistently applying load below the tissue tolerance threshold can accelerate healing via mechanostranduction. If you want to check out a great (and relatively brief) outline of how this process works, check out this great article in the BMJ. Paying careful attention to activities of daily living and work requirements to ensure that tissue capacity isn’t exceeded is also critical for developing an optimal recovery glidepath. Patient education can be especially important for tissues of the lumbar spine, which can experience higher tissue loads with certain mundane activities such as sitting and standing than walking. This issue is what I attribute to highly variable physical therapy outcomes in back pained individuals, but I digress.
The other cool thing about using optimal loading as a paradigm is that it applies to injury prevention as well. This concept explains why the strongest evidence for injury prevention of any training modality is resistance training. It also explains why resistance training enjoys a dose-response relationship with injury prevention in this meta-analysis of randomized controlled trials.
A lot of clinical reasoning centers around magical thinking. This is pretty obvious with eastern medicine justifications for treatments, like acupuncture/meridians, but also applies to the biomedical model as well when it tries to explain complex phenomena in reductive terms without acknowledging that accuracy is being traded for brevity. In order to avoid magical thinking, I like to outline my understanding for the cause and effect relationships surrounding basic concepts like “healing” and “injury”. If that sort of reasoning resonates with you, I encourage you to hang your hat on optimal loading as the simple paradigm you can rely on to guide you through healing from any MSK injuries you might be unfortunate enough to endure. As for how to apply that paradigm, well, just because it’s simple doesn’t mean it’s easy. A good PT can help you identify how you can get through your day without getting overloaded, and provide the right dose of the right exercises to help you beat the timeline that might otherwise be dictated by natural history.
Excellent, very thorough and thoughtful. Although the older me still benefits from this explanation, the younger me who took all the damage needed it more. Like many people who have active lifestyles, I hate doing nothing. So when injured -- even seriously -- I wanted to recover as quickly as possible. But some things as it turns out -- and as you explain very well -- cannot be rushed. But if we accept that and find a balance, and active and productive recovery is possible. I've been guilty of too much black & white thinking in the past. When you can't do what you're used to, sometimes you don't want to do anything. If I had memo to my younger self: be more patient when injured. You can stay active, but give yourself more time than you think you need to fully recover.
Optimal loading below tissue tolerance sounds great but hard to find the area below the curve. I have knee osteoarthritis and was doing strengthening exercises for my quads and gluts. Did too much and walked with a limp for weeks. I know it’s individualized and difficult to find the right loading. And at age 69 do I ever recognize how many months it takes to heal/repair/remodel! GOT to be patient I guess and ignore the surgeons who say “A chance to cut is a chance to heal”……